Over the last twenty years, mindfulness studies have exploded from a handful of curious experiments to a legitimate scientific field with thousands of publications. Back in 2000, you could count serious meditation studies on your fingers. Today, major research universities dedicate entire labs to understanding how sitting quietly and paying attention might rewire your brain or ease chronic pain.
Here's the thing, though: not every study carries equal weight. Some findings come from rigorous trials involving hundreds of participants tracked over years. Others? They're small pilot projects with twenty college students meditating for a week. The quality varies wildly, and that matters when you're trying to figure out if meditation actually works or if we're just seeing hype amplified through social media and wellness marketing.
The challenge is separating solid evidence from preliminary hunches. Certain uses—like managing persistent pain or preventing depression from returning—rest on dozens of well-designed trials. Other applications sound promising but haven't survived careful testing yet.
How Mindfulness Research Is Conducted in Scientific Settings
When scientists study meditation, they face unique challenges that drug researchers don't encounter. You can't exactly give someone a "placebo meditation" without them knowing.
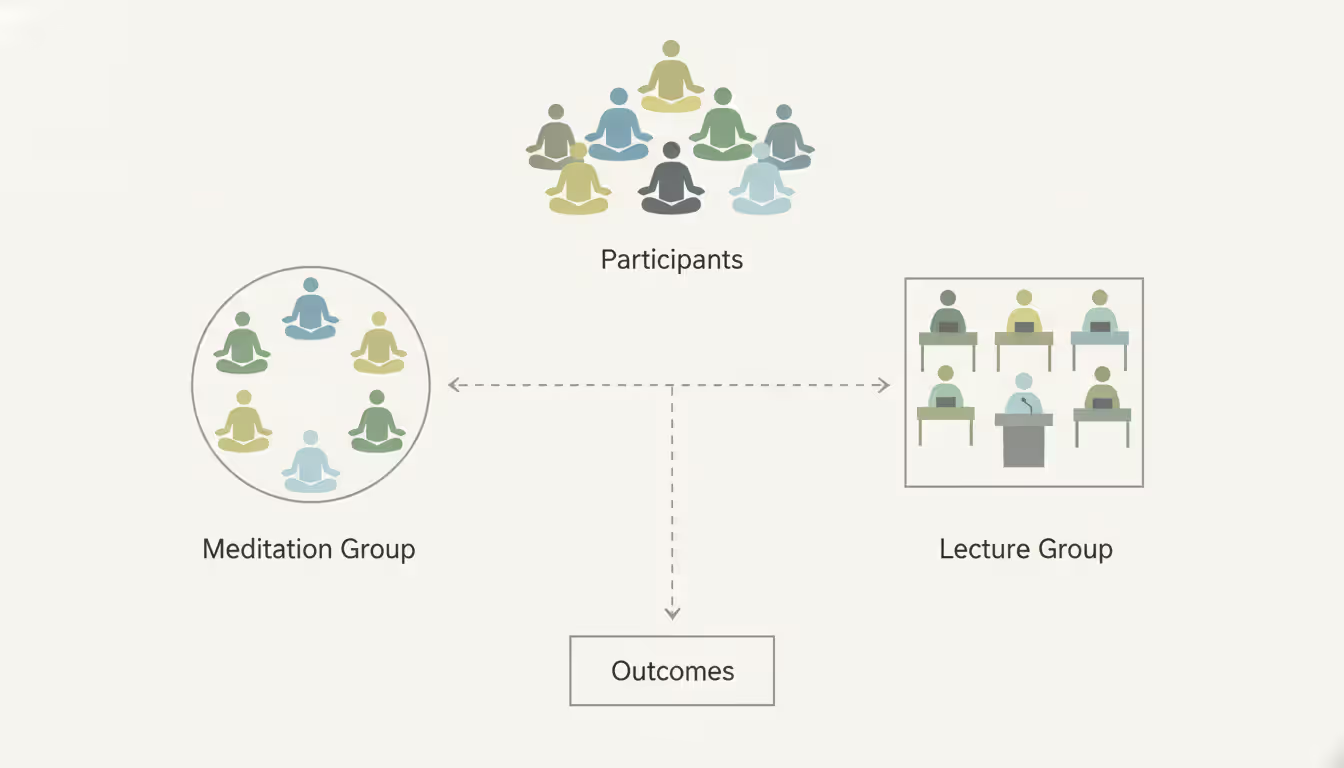
The strongest approach involves randomized controlled trials. Researchers recruit volunteers, then randomly split them into groups. One group learns meditation. The other might attend health education classes, exercise programs, or simply wait their turn (waitlist controls). Random assignment helps ensure the groups are similar at the start, so differences at the end likely stem from the intervention itself.
Sample size creates a major dividing line between weak and strong studies. Those early 1990s papers often tested meditation on 15-25 people—barely enough to detect anything meaningful. Modern research typically enrolls 50-200 participants. Why does this matter? Smaller samples miss subtle effects and can produce fluky results that disappear when you repeat the experiment. A study with 30 people might show meditation reduces anxiety by 40%, but replicate it with 200 people and the effect shrinks to 15% or vanishes entirely.
Author: Ethan Solberg;
Source: 5sensesspa.com
Peer review acts as quality control, though it's imperfect. Before publication, independent experts evaluate the study design, statistics, and conclusions. They catch obvious errors and methodological problems. Still, flawed research slips through, especially in lower-tier journals desperate for content. A paper in JAMA Internal Medicine underwent far more scrutiny than one in the Journal of Obscure Meditation Research (not a real journal, but you get the idea).
Blinding—keeping participants unaware of whether they received the real treatment—proves nearly impossible with meditation. You know if you spent eight weeks learning to watch your breath versus attending nutrition lectures. Some researchers use "active controls" where both groups do something structured and plausible, which helps account for benefits from attention, social interaction, or simply having somewhere to be each week.
Clinical trials differ fundamentally from observational studies. Trials teach meditation to newbies and measure what changes. Observational research compares longtime meditators against non-meditators. The problem? People who've meditated daily for ten years probably differed from non-meditators even before they started. Maybe they're more conscientious, less stressed to begin with, or healthier in ways that have nothing to do with meditation. Observational studies can't prove meditation caused the differences you observe.
Major Findings from Meditation Research Studies
So what have all these studies actually discovered? The clearest wins come from stress research. Dozens of solid trials show meditation lowers cortisol (your main stress hormone) and reduces self-reported stress. The effect isn't huge—meditation won't eliminate stress from a toxic job or dysfunctional relationship—but it's real and replicable.
Depression presents a more nuanced picture. If you've battled major depression multiple times and recovered, meditation can slash your chances of relapse by roughly half. That's comparable to staying on antidepressants long-term. The catch? Meditation works better for preventing depression's return than treating an active episode. When you're in the depths of depression right now, medication and traditional therapy typically outperform meditation.
Anxiety shows moderate improvements across numerous studies. People with generalized anxiety disorder (constant worry about everything) tend to respond well. Social anxiety and panic attacks? Results vary more widely. Some folks get substantial relief; others notice minimal change. We still can't predict who'll benefit most.
Chronic pain represents perhaps meditation's strongest application. Here's what's fascinating: meditation often doesn't reduce pain intensity much. Your back still hurts, your joints still ache. What changes is your relationship to the pain—how much it bothers you, how much you catastrophize about it, whether it ruins your entire day. Patients report the same pain levels but significantly less suffering. They function better, sleep better, need fewer opioids.
Meditation Style
What Researchers Study Most
Published Studies (Approximate)
Key Findings
Common Study Length
Mindfulness Meditation
Stress responses, recurring depression, general anxiety
2,000+
Less rumination, better emotional control, lower stress reactivity
8 weeks (45 min/day)
Transcendental Meditation
Heart health, blood pressure, anxiety symptoms
400+
Modest BP reduction, decreased anxiety, better sleep
20 min twice daily, tracked 3-6 months
Loving-Kindness Meditation
Compassion, social bonds, positive emotions
150+
More positive feelings, increased empathy, reduced unconscious bias
6-8 weeks
Body Scan
Chronic pain, body awareness, insomnia
300+
Stronger mind-body connection, less pain catastrophizing, improved sleep quality
8-12 weeks
Physical health outcomes get murkier. Blood pressure drops in some trials but not others. Immune markers like inflammatory proteins sometimes improve, particularly if you're already stressed. Cancer patients who meditate report better quality of life—less anxiety, fatigue, nausea during chemo—but meditation doesn't shrink tumors or extend survival based on current evidence.
Cognitive benefits skew toward older adults. Seniors who meditate show better attention spans and working memory compared to non-meditating peers. Younger people show smaller gains, probably because they're already performing near their cognitive peak. A few studies suggest meditation slows normal age-related brain shrinkage, though this finding needs confirmation from larger trials.
Mindfulness Applications in Healthcare Settings
Walk into Massachusetts General Hospital, the Cleveland Clinic, or Mayo Clinic today, and you'll find dedicated mindfulness programs. This wasn't true fifteen years ago. What changed? Accumulated research convinced administrators that evidence-based mindfulness programs deliver measurable benefits at reasonable costs.
The flagship program, Mindfulness-Based Stress Reduction (MBSR), originated at UMass Medical School in the 1970s. It follows a standardized eight-week format: weekly group sessions teaching meditation, gentle yoga, and group discussion, plus daily home practice. Hospitals now deploy MBSR for conditions ranging from fibromyalgia and irritable bowel syndrome to psoriasis and cancer-related distress.
Pain clinics increasingly treat meditation as standard care alongside medications and physical therapy. Instead of replacing conventional treatments, meditation augments them. Patients learn body scanning and breath awareness to modulate pain perception. This matters financially too—some insurers now cover these programs after seeing reduced ER visits and lower opioid prescriptions.
Cardiac rehab programs traditionally focused on exercise and diet. Now many add meditation to the mix. Heart attack survivors who practice meditation consistently show fewer subsequent cardiac events in follow-up studies. Whether meditation directly protects your heart or simply correlates with healthier choices (meditators might also eat better, exercise more, manage stress differently) remains unclear.
Oncology departments offer meditation specifically for symptom management during treatment. Research shows cancer patients who meditate regularly experience less severe nausea, fatigue, and anxiety. Sleep quality often improves too, which matters since insomnia spikes during chemotherapy.
Psychiatric settings move more cautiously. Outpatient therapists frequently teach mindfulness skills as part of treatment. Inpatient psychiatric units? They're warier. Some people with psychotic disorders or severe trauma report worse symptoms when they meditate, particularly during acute crises. Clinics now screen patients carefully before recommending meditation.
Prenatal care has embraced mindfulness more recently. Pregnant women who complete meditation programs report lower anxiety and fewer depressive symptoms during pregnancy. Small studies hint at possible benefits for birth outcomes—potentially fewer preterm deliveries—but larger trials haven't confirmed this yet.
What Cognitive Science Reveals About Meditation Effects
Brain imaging transformed meditation research from subjective self-reports to objective measurements. When scientists can photograph your brain structure or watch activity patterns in real-time, the conversation shifts.
Long-term meditators show measurably thicker prefrontal cortex tissue—the brain region handling executive functions like planning, emotional regulation, and impulse control. This finding has held up across multiple studies using different meditation styles and scanning technologies. The thickness increase correlates with practice hours: more meditation, more tissue. Still, correlation doesn't prove causation. Maybe people born with thicker prefrontal cortices naturally gravitate toward meditation?
Neuroplasticity—the brain's ability to reorganize itself—continues throughout adulthood, and meditation appears to harness this capacity. Studies document strengthened connections between attention-control regions and weakened connections in the default mode network (the brain circuits that activate during mind-wandering and self-focused rumination).
Author: Ethan Solberg;
Source: 5sensesspa.com
Attention mechanisms definitely change with practice. Experienced meditators maintain focus longer during boring tasks and bounce back faster after distractions. EEG studies reveal altered brainwave patterns—more alpha and theta waves associated with relaxed alertness. These patterns persist somewhat even when not actively meditating.
Memory effects vary by meditation type. Mindfulness practice seems to expand working memory capacity—your ability to temporarily hold and manipulate information. Older adults benefit most here. Some research suggests meditation slows hippocampal shrinkage that normally accompanies aging, though this finding remains controversial.
The amygdala—your brain's threat detector and emotional alarm system—shows reduced activation when meditators view disturbing images. This dampened response might explain why practitioners report less anxiety and emotional reactivity. Structural scans show smaller amygdala volume in long-term meditators, though whether this represents beneficial adaptation or something else entirely sparks debate.
Interoceptive awareness (perceiving internal bodily states like heartbeat or muscle tension) sharpens with meditation. Brain regions like the insula show heightened activation when meditators focus on physical sensations. This enhanced body awareness potentially contributes to emotional regulation, since emotions manifest partly through bodily changes.
The default mode network—active during self-referential thinking and mental time travel—shows decreased activity during meditation. This network's connectivity patterns change in experienced practitioners, which some researchers link to reduced rumination and self-focused worry.
Psychology Research on Mindfulness Interventions
Psychological research has generated specific therapeutic applications with varying evidence quality. Two programs dominate the landscape: MBSR (described earlier) and Mindfulness-Based Cognitive Therapy (MBCT).
MBCT emerged from combining mindfulness training with cognitive therapy elements, specifically targeting recurrent depression. The program teaches people to spot early warning signs of depression and respond skillfully instead of automatically spiraling. Multiple large trials demonstrate MBCT cuts relapse rates by 40-50% in people who've experienced three or more previous depressive episodes. This evidence proved strong enough that clinical guidelines in the UK, Canada, and several other countries now recommend MBCT as a first-line strategy for preventing depression's return.
Anxiety disorders respond inconsistently. Generalized anxiety disorder consistently improves across studies, with effect sizes matching cognitive-behavioral therapy. Social anxiety shows moderate benefits. Panic disorder produces mixed results—some people improve dramatically while others experience heightened anxiety when focusing attention on bodily sensations that trigger panic attacks.
Author: Ethan Solberg;
Source: 5sensesspa.com
PTSD research reveals a complicated landscape. Some trauma survivors benefit from mindfulness practice. Others find meditation triggers intrusive memories or dissociative states. Trauma-informed modifications—keeping eyes open, emphasizing participant choice and control, avoiding extended silence—appear safer than standard protocols. Current evidence suggests mindfulness works best for PTSD when combined with trauma-focused therapy rather than used standalone.
Substance use disorders attract growing research attention. Mindfulness-based relapse prevention teaches people to ride out cravings without acting on them—surfing the urge rather than fighting it or surrendering to it. Studies show reduced substance use and longer abstinence periods compared to standard aftercare. The approach appears particularly effective for marijuana and alcohol dependence, with weaker evidence for opioid and stimulant addiction.
Eating disorders represent newer territory. Mindful eating interventions help people with binge eating disorder and bulimia by increasing awareness of hunger and fullness cues. Initial studies look promising, though sample sizes remain small and long-term outcomes need investigation.
ADHD research yields frustratingly inconsistent findings. Some studies report improved attention and reduced impulsivity in children and adults with ADHD who practice meditation. Others show minimal benefits. The obvious challenge: maintaining consistent meditation practice when your core symptoms include difficulty sustaining attention and following through on intentions.
The research on mindfulness is still in its infancy, but the evidence base is growing exponentially. What we're learning is that the systematic training of attention and awareness can have profound effects on the body, the mind, and their interconnectedness—effects that are now measurable and increasingly well understood
— Jon Kabat-Zinn
Common Limitations in Current Meditation Studies
Despite improving methodology, meditation research carries persistent flaws that should temper your confidence in findings.
Sample bias saturates the field. Studies recruit volunteers interested in meditation, creating self-selection problems. People who volunteer for meditation studies probably differ from the general population in motivation, openness to contemplative practices, and baseline mental health. This makes it tough to predict how meditation might work for skeptical or unmotivated people—probably the majority of the population.
Control group selection presents ongoing headaches. What counts as a fair comparison? Waitlist controls (participants receive nothing while waiting) fail to account for placebo effects or benefits from attention and social support. Active controls like health education classes provide better comparisons but raise new questions: Are differences due to meditation specifically or because meditation is simply more engaging than sitting through lectures on nutrition?
Expectancy effects muddy the waters. Participants who believe meditation will help often report improvements regardless of actual practice. Some studies attempt controlling for expectations by describing meditation neutrally or comparing it with interventions presented as equally beneficial. These approaches help but don't eliminate expectancy bias.
Measurement challenges plague the field. Self-report questionnaires—the most common outcome measure—suffer from social desirability bias and subjective interpretation. Biological measures like cortisol levels or brain scans provide objective data but don't necessarily correlate with subjective well-being. What matters more: measurable brain changes or whether someone actually feels less anxious?
Replication problems have surfaced as the field matured. Several high-profile findings failed to replicate in larger, better-controlled studies. Early claims about dramatic immune function boosts or major personality transformations haven't held up under scrutiny. Publication bias favors positive findings—journals prefer publishing "meditation works!" over "meditation showed no effect"—meaning failed replications often languish unpublished, painting an overly rosy picture.
Funding constraints limit study quality. Large-scale trials with adequate sample sizes, multi-year follow-ups, and rigorous controls require serious money. Most meditation research survives on small grants or institutional funding insufficient for optimal designs. Pharmaceutical companies invest billions in drug trials; meditation research operates on a fraction of one percent of that budget.
Dosage questions remain unanswered. How much meditation produces benefits? Studies use wildly varying protocols—from ten minutes daily to multi-day retreats—making dose-response relationships impossible to establish. Individual differences in optimal dosage likely exist but haven't been systematically investigated.
Mechanism uncertainty persists. Even when meditation produces measurable benefits, researchers often can't pinpoint why. Is it the specific technique? The quiet time away from screens and demands? Social support from group classes? Lifestyle changes that accompany meditation practice? Some combination? Identifying active ingredients would help optimize interventions but proves methodologically nightmarish.
FAQ
How reliable is current mindfulness research?
Reliability spans a wide range depending on the specific study. Large randomized trials published in journals like JAMA Psychiatry or Psychological Medicine offer trustworthy evidence. Small pilot studies with 20 participants or observational research should be viewed skeptically. Meta-analyses combining multiple studies provide stronger conclusions than individual papers. For chronic pain, depression relapse prevention, and stress reduction, the research quality is quite good—dozens of well-designed trials pointing in the same direction. For other applications like ADHD or acute PTSD treatment, evidence remains preliminary and inconsistent.
What health conditions have the strongest research support for meditation?
Three areas stand out with robust evidence: chronic pain management, preventing depression relapse in people with recurrent episodes, and general stress reduction. Generalized anxiety disorder also shows consistent benefits across multiple high-quality trials. Moderate evidence supports meditation for irritable bowel syndrome, insomnia, and high blood pressure, though more research would strengthen confidence. Weaker or inconsistent evidence exists for ADHD, treating active depression (versus preventing relapse), and using meditation as standalone PTSD treatment.
How long does meditation need to be practiced to see research-backed results?
Most clinical trials use eight-week programs with daily practice ranging from 20-45 minutes. Measurable changes in stress, anxiety, and mood typically appear within four to six weeks of consistent practice. Brain structure changes visible on MRI scans generally require months to years of regular meditation. That said, individual variation is enormous. Some people notice subjective benefits within days or weeks. Others practice for months without perceiving any effects. Research-based averages don't reliably predict individual outcomes—you might respond faster or slower than the typical participant.
Are there any risks identified in meditation research studies?
Yes, though serious adverse effects appear relatively uncommon in research settings. Roughly 10-15% of meditation practitioners report negative experiences including increased anxiety, disturbing intrusive thoughts, or emotional numbness. People with trauma histories, psychotic disorders, or severe depression face elevated risks. Some individuals experience dissociation or depersonalization during meditation. Extended silent retreats carry higher risk than brief daily sessions. Proper screening and qualified instruction reduce but don't eliminate potential adverse effects. If you have significant mental health concerns, consult a therapist before starting meditation practice.
How can I tell if a meditation study is credible?
Check several factors. First, was it published in a peer-reviewed journal? Second, look for randomized controlled designs rather than observational studies comparing existing meditators to non-meditators. Third, larger sample sizes (at least 50 participants, preferably more) provide more reliable results than small pilot studies. Fourth, examine the control group—waitlist controls are weaker than active comparison conditions. Fifth, look for objective outcome measures beyond self-report questionnaires. Sixth, be skeptical of dramatic claims or studies funded by organizations with commercial interests in promoting meditation. University-based research generally maintains higher standards than industry-funded studies, though exceptions exist.
What gaps still exist in mindfulness research?
Major gaps include limited understanding of who benefits most and who might experience adverse effects. We can't yet predict individual responses reliably. Optimal dosage remains unclear—how much practice produces maximum benefit with minimum time investment? Long-term outcomes beyond one or two years are rarely studied; we don't know if benefits persist five or ten years later. Mechanisms of action need clarification: exactly why and how does meditation produce its effects? Research on children and adolescents lags far behind adult studies. Most research examines Western, educated populations; cross-cultural studies are scarce. Comparative effectiveness research—which meditation type works best for specific conditions—remains underdeveloped.
Scientific investigation of mindfulness has come a long way from its fringe beginnings. We now have thousands of peer-reviewed studies documenting measurable effects on brain structure, psychological well-being, and physical health. The strongest evidence clusters around chronic pain management, stress reduction, and depression relapse prevention, with emerging support for numerous other applications.
But significant limitations remain. Small sample sizes, methodological challenges, and replication failures remind us this field is still developing. Meditation doesn't work for everyone, and some people experience adverse effects that rarely make headlines. The gap between popular claims (meditation as miracle cure!) and actual research findings stays frustratingly wide.
Healthcare integration reflects growing confidence in what we've learned. Hospitals run meditation programs. Insurance companies cover them. Clinical guidelines recommend mindfulness interventions for specific conditions. This mainstream acceptance stems from accumulated evidence demonstrating real benefits—modest perhaps, but real and replicable.
Future research will likely clarify optimal applications, identify who benefits most, and explain mechanisms of action more precisely. As neuroimaging technology advances and study designs improve, our understanding will deepen. For now, the evidence suggests meditation offers genuine benefits for many people, while acknowledging that individual responses vary widely and scientific understanding remains incomplete. Not a magic bullet, but a legitimate tool worth considering for certain conditions and populations.
Transform your mornings with guided meditation podcasts. This comprehensive guide covers the best free options, how to build a sustainable routine, and what makes quality meditation audio. Compare popular podcasts and learn practical tips for fitting mindfulness into busy schedules and commutes
Discover practical meditation techniques you can use at your desk to boost work performance. Learn how successful entrepreneurs integrate mindfulness into their workday, improve decision-making, and build sustainable practices without disrupting workflow
Becoming a meditation teacher requires structured training in pedagogy, ethics, and techniques. With hundreds of programs available in 2026, choosing the right meditation teacher training determines your professional credibility and earning potential. Learn how to evaluate programs, avoid common mistakes, and launch your teaching career
Most people abandon meditation within three weeks. The difference between those who quit and those who maintain a practice for years comes down to how they structure their approach. Discover realistic strategies for building meditation routines that survive contact with busy schedules
The content on this website is provided for general informational and educational purposes only. It is intended to explain concepts related to meditation, mindfulness, mental health, and spiritual practices.
All information on this website, including articles, guides, and examples, is presented for general educational purposes. Meditation outcomes may vary depending on individual practices, health conditions, and guidance.
This website does not provide medical, mental health, or spiritual advice, and the information presented should not be used as a substitute for consultation with qualified professionals.
The website and its authors are not responsible for any errors or omissions, or for any outcomes resulting from decisions made based on the information provided on this website.